Below is a summary of the data submitted to the NDRLS since 2011.
If you are conducting a publicly funded research project and would like to gain access to an anonymised version of the NDRLS MDCT dataset, please contact the NDRLS team.
NDRLS MDCT survey participation
Facility registrations
Figure 1 and Figure 2 show the date that facilities currently registered with the NDRLS first registered. The colours in Figure 1 and Figure 2 categorise the facilities by state/territory and facility type respectively.
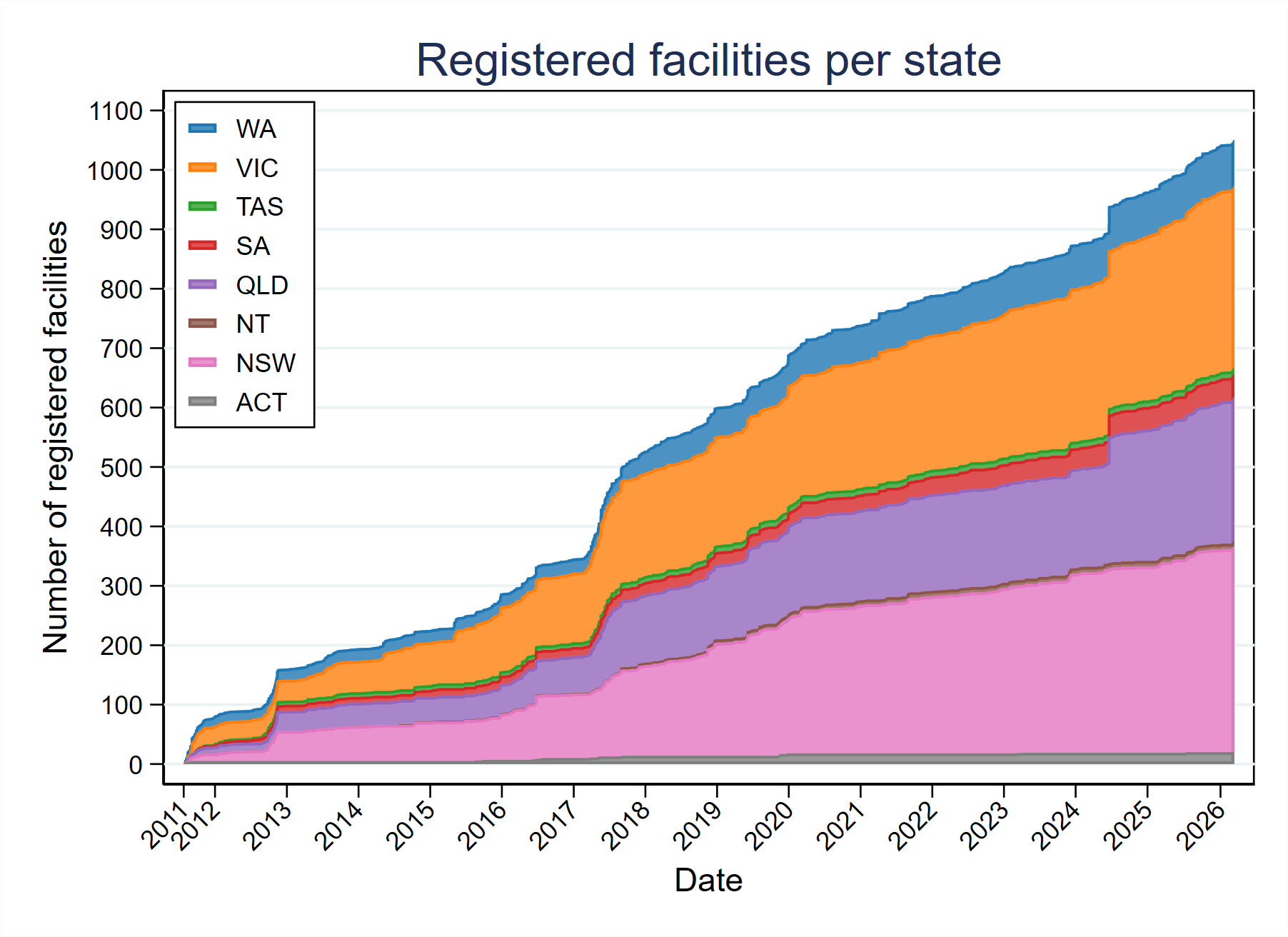
Figure 1: Area plot showing the number of facilities registered with the NDRLS MDCT survey, categorised by state
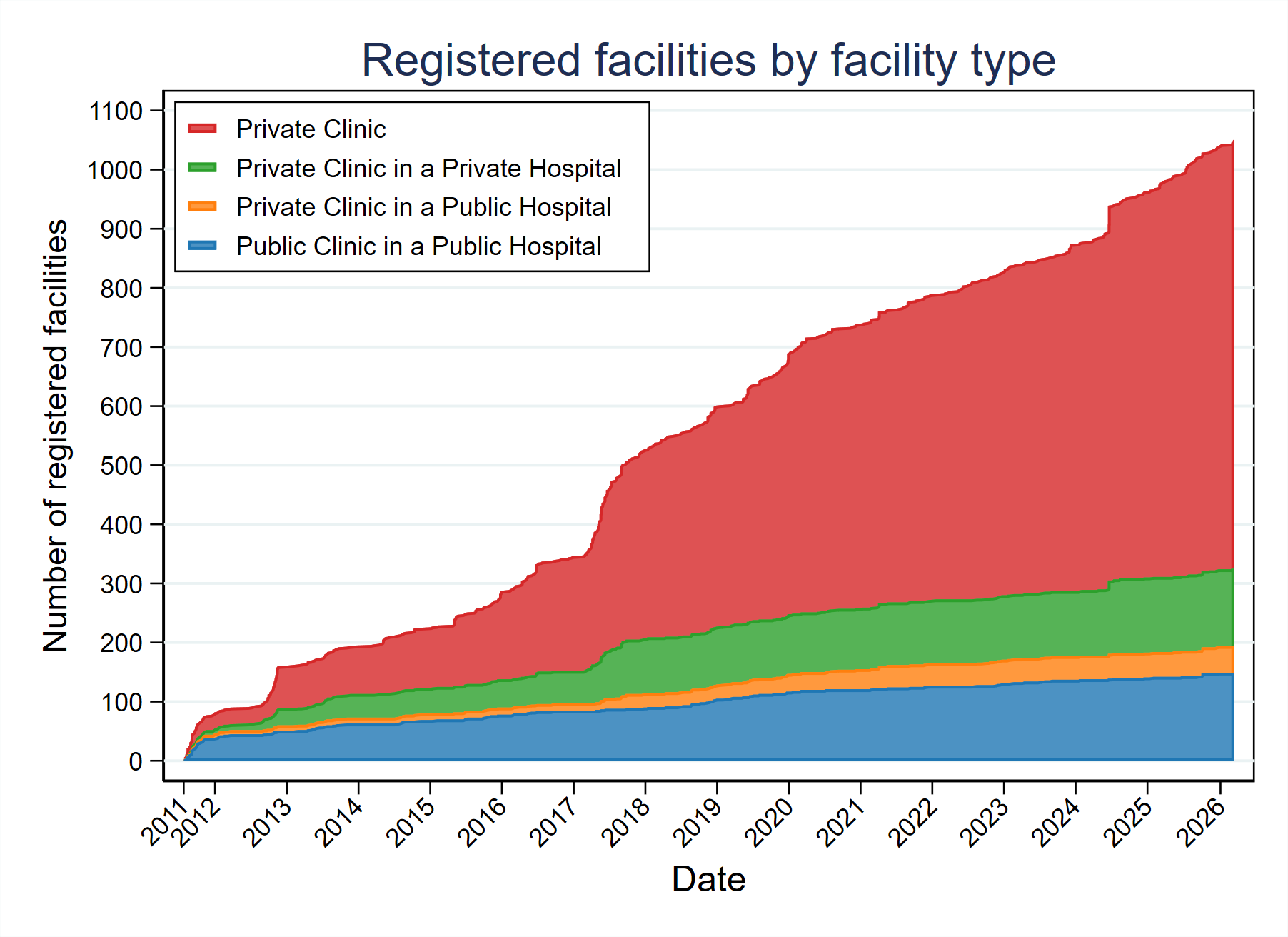
Figure 2: Area plot showing the number of facilities registered with the NDRLS MDCT survey, categorised by the type of facility
Number of surveys submitted
Table 1 shows the number of surveys submitted to the NDRLS since August 2011 (the start of the service), categorised by protocol and age group.
Table 1: Number of surveys submitted to the NDRLS MDCT survey, categorised by age group, protocol and year
| Age group | Protocol | 2011 | 2012 | 2013 | 2014 | 2015 | 2016 | 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | 2023 | 2024 | 2025 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Adult (15+ years) surveys submitted | Head | 56 | 113 | 166 | 147 | 202 | 284 | 465 | 591 | 712 | 729 | 555 | 599 | 614 | 687 | 717 | 6637 |
| Neck | 30 | 57 | 80 | 76 | 141 | 192 | 358 | 131 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 1065 | |
| Soft-tissue neck | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 259 | 453 | 530 | 353 | 396 | 439 | 505 | 543 | 3478 | |
| Cervical spine | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 315 | 565 | 597 | 459 | 508 | 526 | 592 | 648 | 4210 | |
| Chest | 44 | 78 | 112 | 113 | 177 | 258 | 422 | 542 | 652 | 682 | 514 | 568 | 591 | 658 | 684 | 6095 | |
| Chest-abdomen-pelvis | 40 | 68 | 100 | 93 | 135 | 200 | 368 | 467 | 559 | 620 | 444 | 493 | 518 | 583 | 609 | 5297 | |
| Abdomen-pelvis | 51 | 100 | 150 | 128 | 194 | 274 | 442 | 575 | 676 | 693 | 549 | 583 | 608 | 671 | 697 | 6391 | |
| Kidney-ureter-bladder | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 256 | 479 | 521 | 408 | 462 | 485 | 549 | 602 | 3762 | |
| Lumbar spine | 34 | 75 | 116 | 105 | 156 | 237 | 419 | 517 | 659 | 672 | 516 | 554 | 567 | 645 | 677 | 5949 | |
| Paranasal Sinuses | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 372 | 372 | |
| Low dose Chest | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 240 | 240 | |
| Total | 255 | 491 | 724 | 662 | 1005 | 1445 | 2474 | 3653 | 4755 | 5044 | 3798 | 4163 | 4348 | 4890 | 5789 | 43496 | |
| Child (5-14 years) surveys submitted | Head | 0 | 28 | 26 | 19 | 22 | 22 | 16 | 10 | 10 | 10 | 10 | 7 | 14 | 8 | 2 | 204 |
| Chest | 0 | 7 | 8 | 7 | 8 | 9 | 13 | 5 | 3 | 6 | 4 | 3 | 3 | 3 | 0 | 79 | |
| Abdomen-pelvis | 0 | 3 | 6 | 4 | 6 | 5 | 6 | 2 | 2 | 4 | 3 | 4 | 5 | 6 | 0 | 56 | |
| Total | 0 | 38 | 40 | 30 | 36 | 36 | 35 | 17 | 15 | 20 | 17 | 14 | 22 | 17 | 2 | 339 | |
| Baby (0-4 years) surveys submitted | Head | 0 | 20 | 23 | 18 | 17 | 20 | 13 | 10 | 6 | 8 | 9 | 5 | 12 | 9 | 1 | 171 |
| Chest | 0 | 3 | 5 | 4 | 3 | 4 | 6 | 3 | 3 | 3 | 3 | 2 | 4 | 4 | 0 | 47 | |
| Abdomen-pelvis | 0 | 0 | 2 | 2 | 1 | 2 | 2 | 1 | 2 | 2 | 2 | 2 | 1 | 1 | 0 | 20 | |
| Total | 0 | 23 | 30 | 24 | 21 | 26 | 21 | 14 | 11 | 13 | 14 | 9 | 17 | 14 | 1 | 238 |
FRL distributions
The curves below show the cumulative distributions for the DLP and CTDIvol from adult abdomen pelvis DRL surveys submitted in 2025. The y-axis displays the percentage of facilities that achieved an FRL below the dose specified on the x-axis.
The blue curve represents all of the submitted data, the orange curve represents the surveys where iterative reconstruction (IR) was used and the green curve represents the surveys where filtered back projection (FBP) was used. The national DRL was derived from data submitted in earlier years and, consequently, the DRLs do not match the 75th percentile of the plotted distributions.
View similar plots for the other protocols.
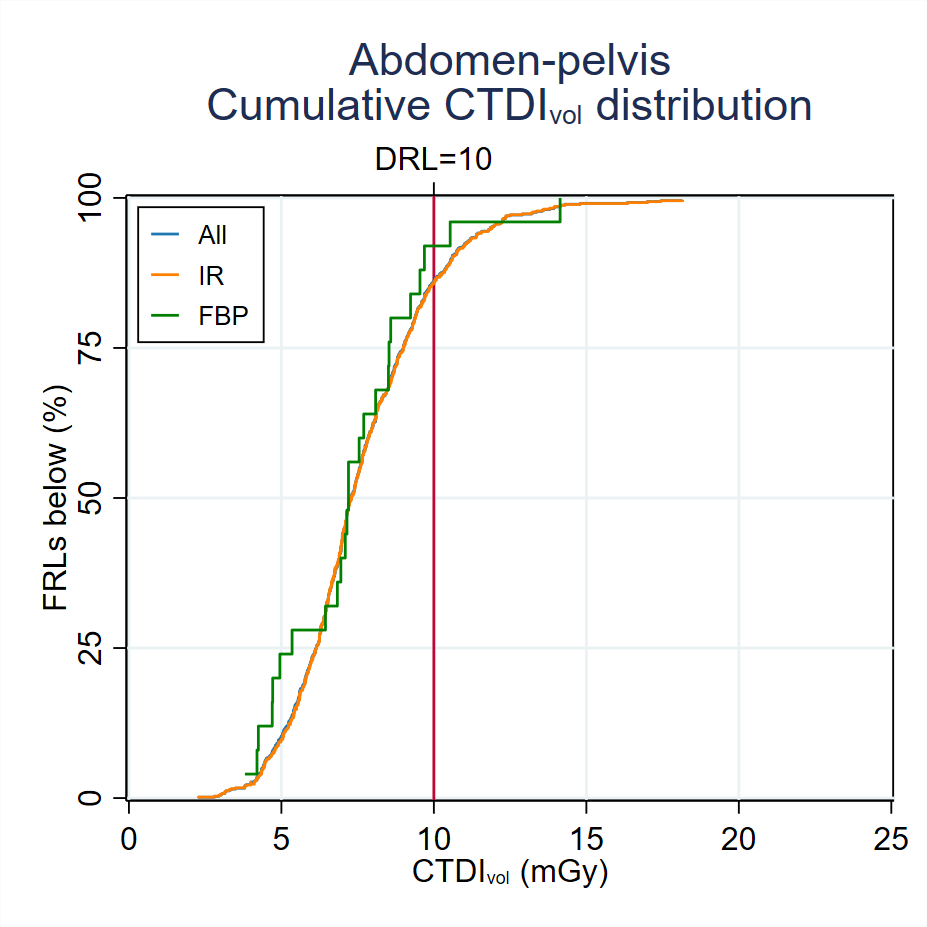
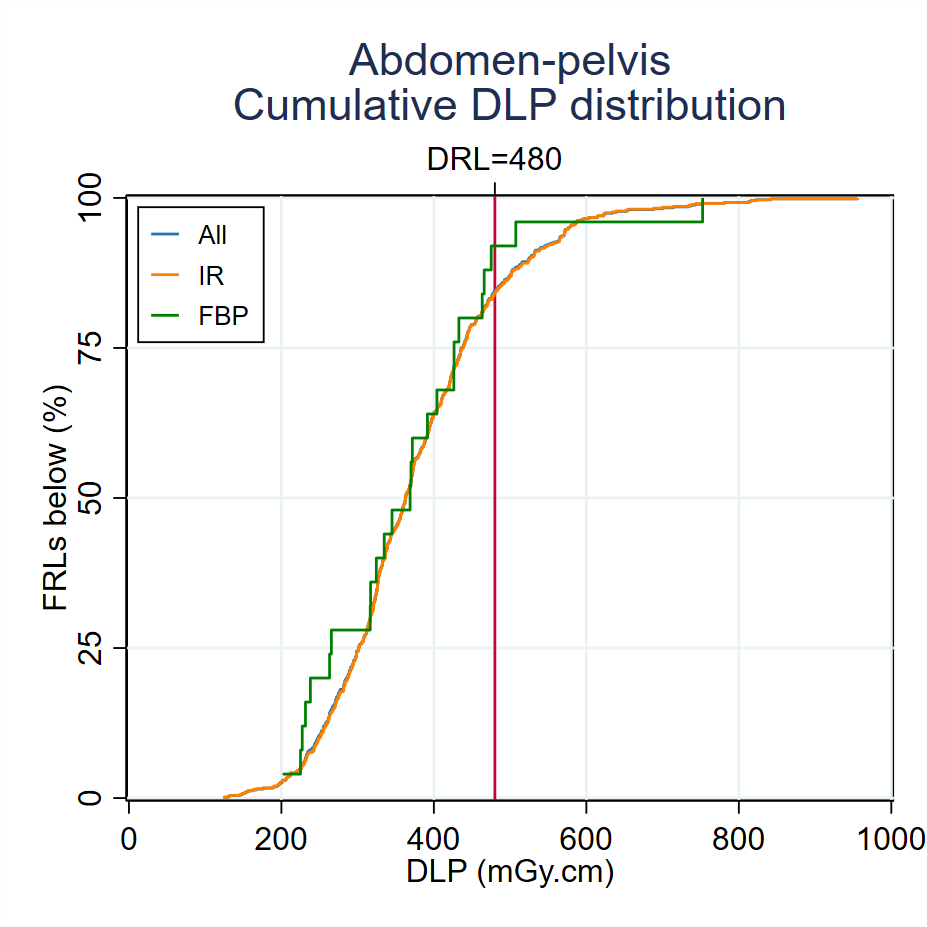
Figure 3: Cumulative dose distributions for abdomen pelvis scans conducted on adult patients. The y-axis provides the percentage of facilities that achieved an FRL below the dose specified on the x-axis. The blue, orange and green curves represent all data, data from scans that used iterative reconstruction (IR) and scans that used filtered back projection (FBP) respectively.
FRL distribution variation over time
Figure 4 shows the change in the median of the FRL distribution since the beginning of 2012 for adult abdomen pelvis scans. The graph has been generated by examining the surveys submitted during a moving 12-month period, where the start and end points of the window have been shifted by daily intervals. The x-axis is the end date of the 12-month interval, the blue line is the median of the corresponding FRL distribution, the red line denotes the current DRL and the light blue region indicates the 25th – 75th percentile range.
View similar graphs for the other adult FRL distributions.
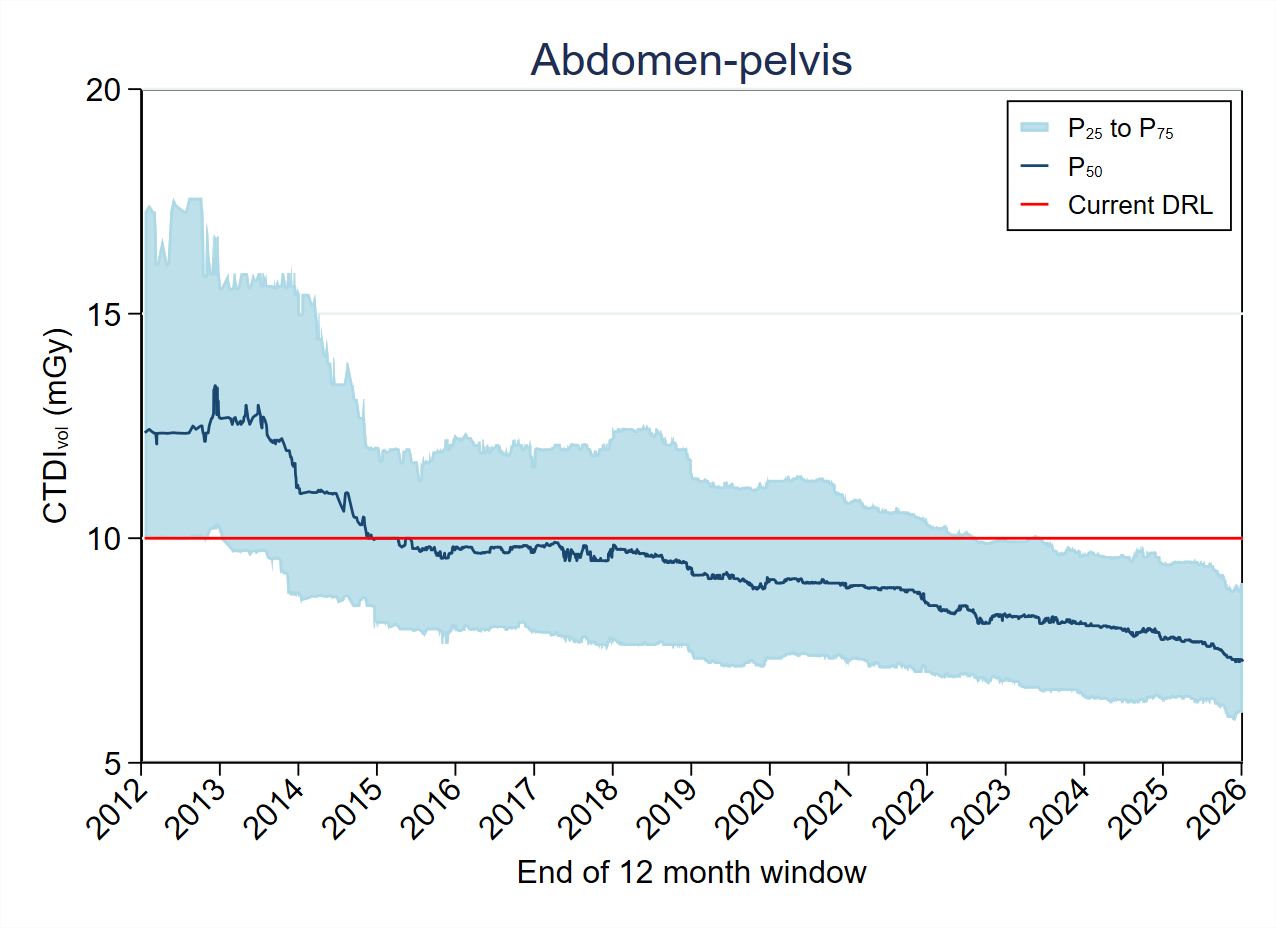
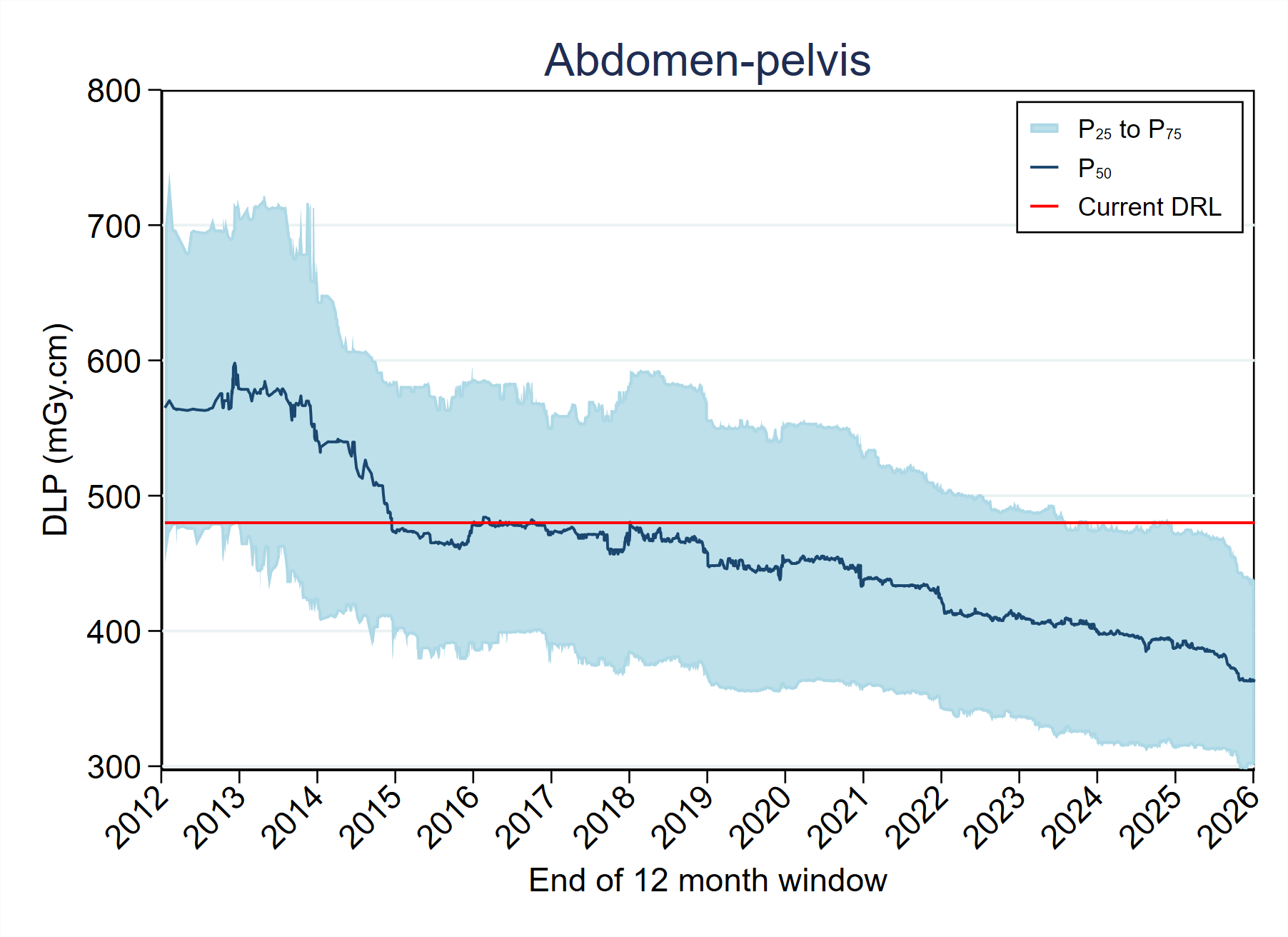
Figure 4: Change in the 75th percentile (P75) of the DLP and the CTDIvol for abdomen pelvis scans. The date along the x-axis denotes the end of the 12-month window of data used to calculate the percentile. The red line represents the current DRL.
Impact of iterative reconstruction
The reductions in the 75th percentile of the FRL distribution can be partially attributed to the increased adoption of iterative reconstruction (IR) techniques. Figure 5 shows the number of surveys submitted since April 2013, categorised by the use of IR.
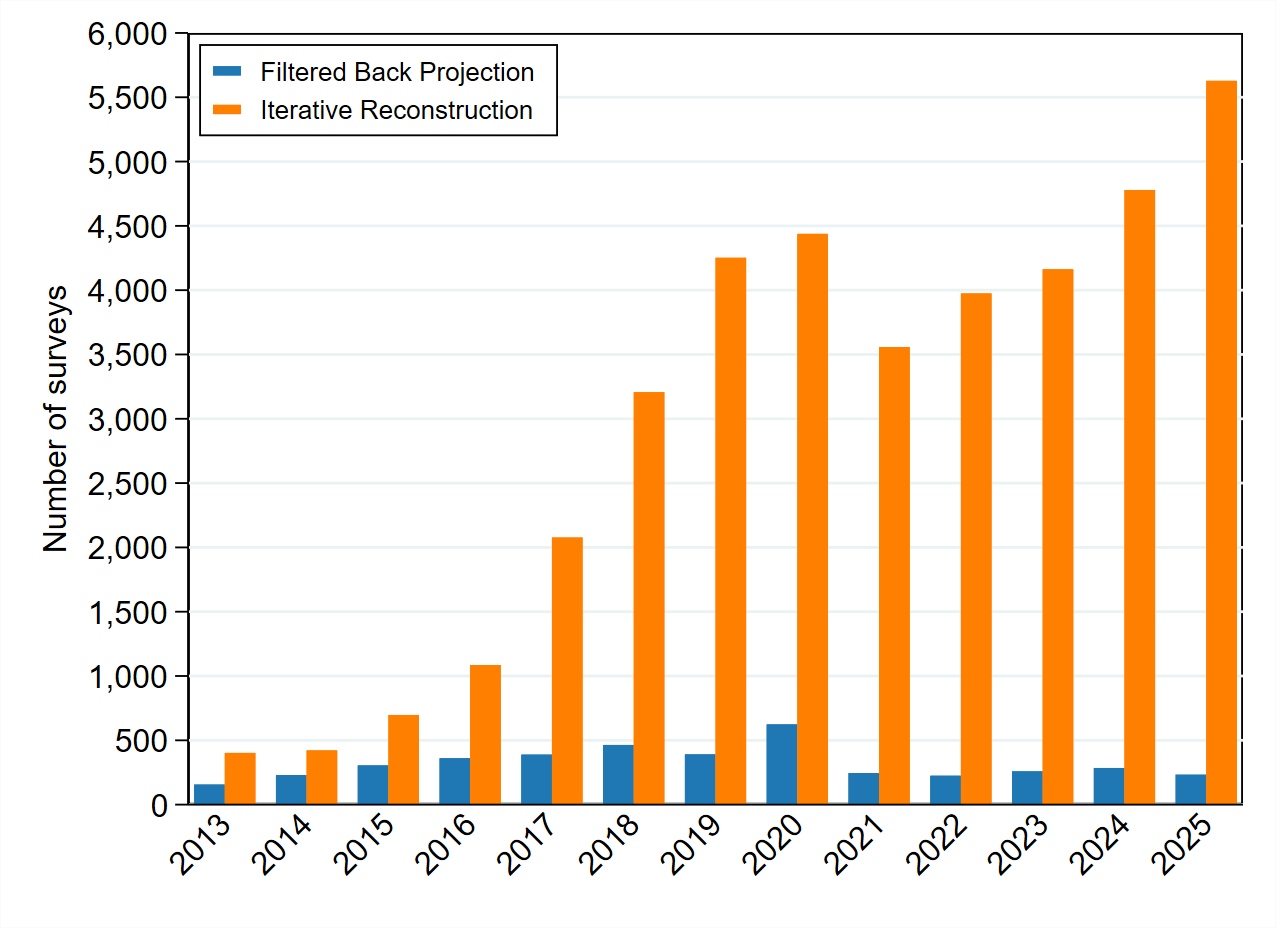
Figure 5: Number of surveys submitted since April 2013, categorised by the use of iterative reconstruction (IR) or filtered back projection (FBP)
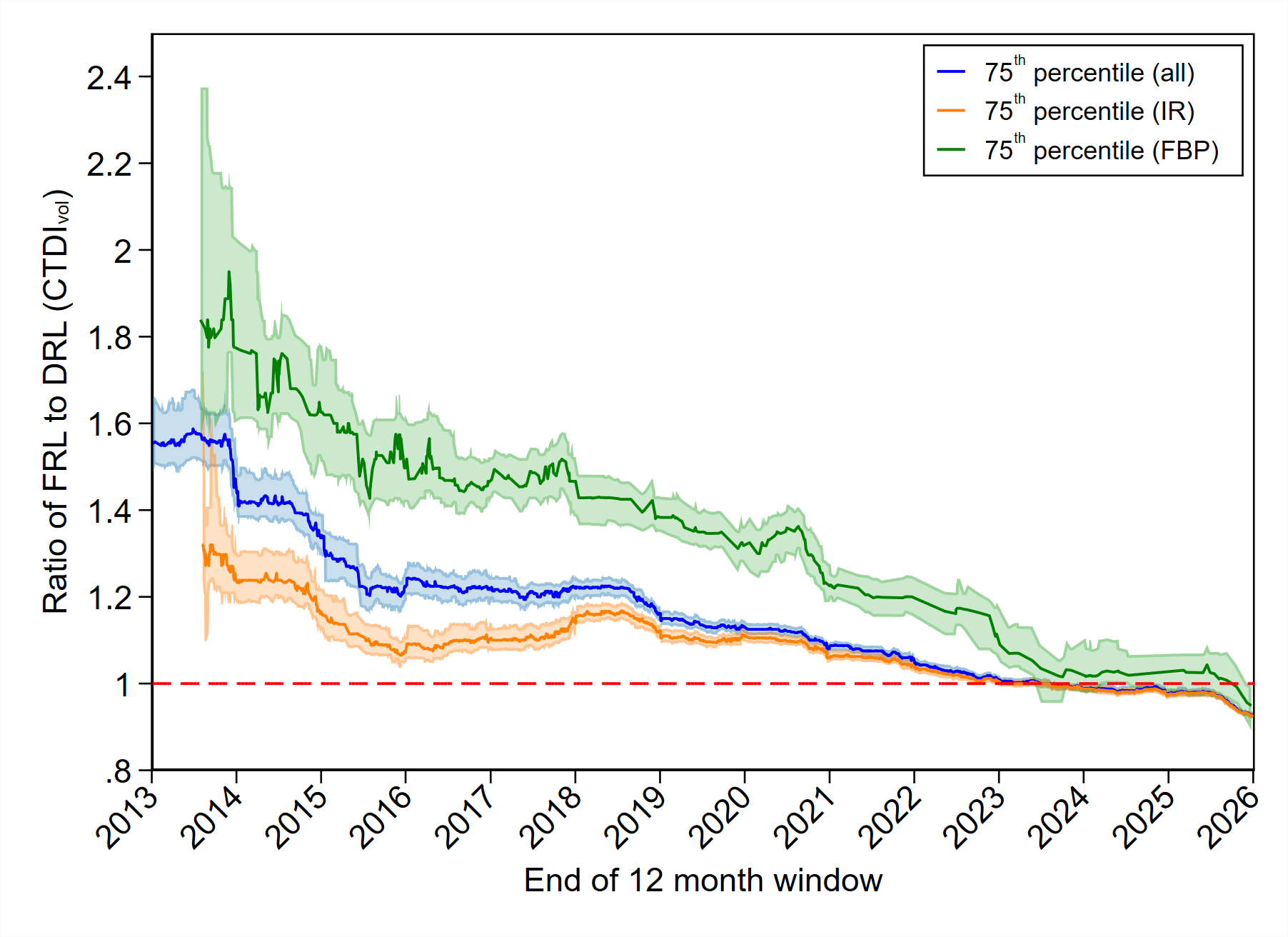
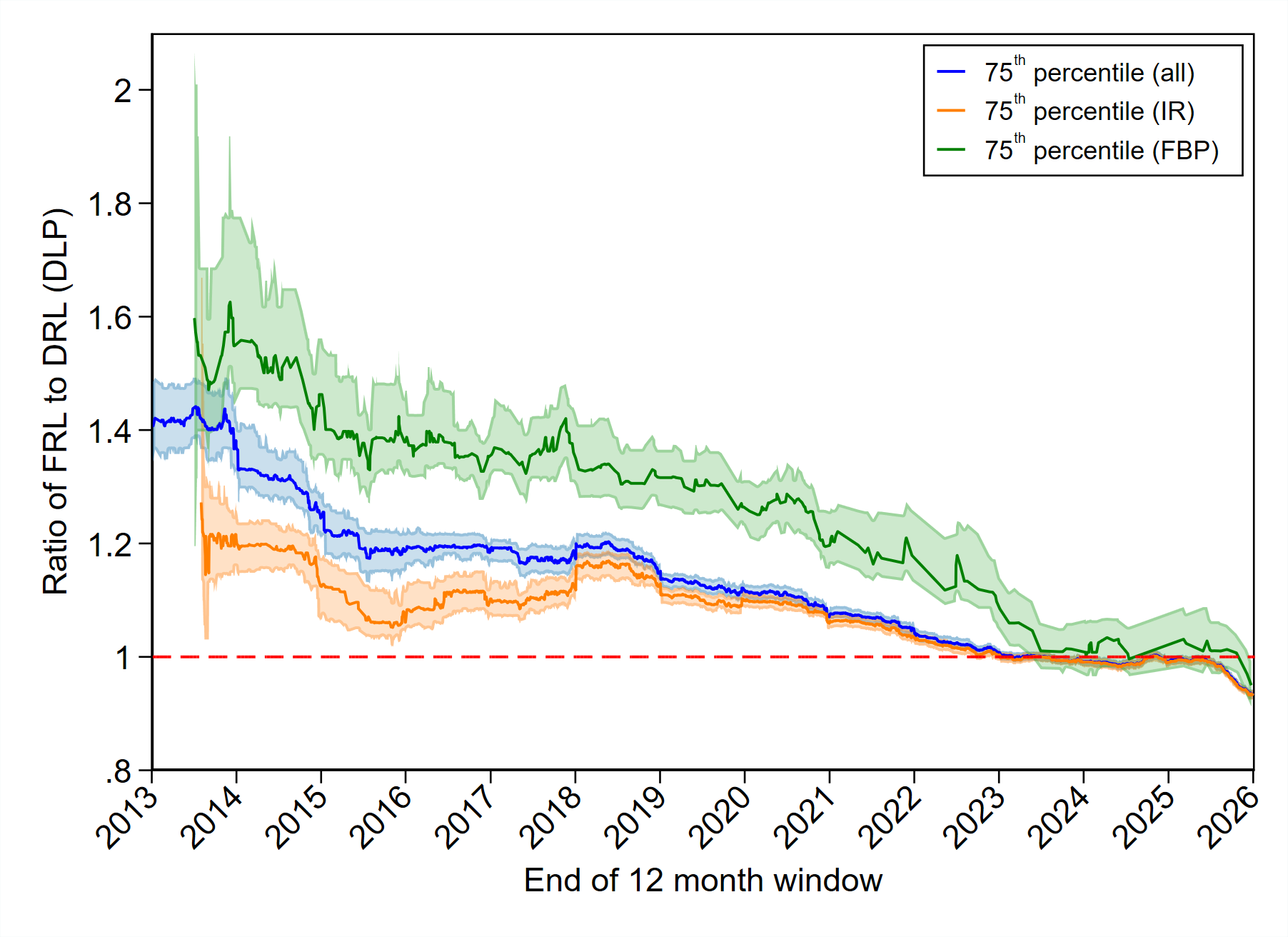
The change in dose distributions is represented in Figure 6 below. The metric plotted is the 75th percentile of the submitted FRLs, where the FRL has been expressed as a fraction of the relevant DRL. The date along the x-axis represents the end of a 12-month period for which the percentile has been calculated. The plot only includes data for protocols where data has been collected from 2013 to 2025 (inclusive).